


A Report Series on Lessons Learned from PEPFAR’s Success
Introduction
No global development program funded by U.S. taxpayers has used data more effectively than the President’s Emergency Plan for AIDS Relief (PEPFAR). A clear hallmark of PEPFAR for two decades has been investing in the granularity of data collection to improve the outcomes and impact of programming and ensure the inclusion of men, women, and children of all ages. Using accurate, localized data for decision-making has been in PEPFAR’s DNA since the beginning and remains at the center of the program’s culture and approach.
We are focusing on a data-driven approach that strategically targets populations at greatest risk in geographic areas with the highest HIV burden. PEPFAR will prioritize prevention, care, and treatment services in the areas of highest HIV incidence.
— PEPFAR Annual Report to Congress for 2015
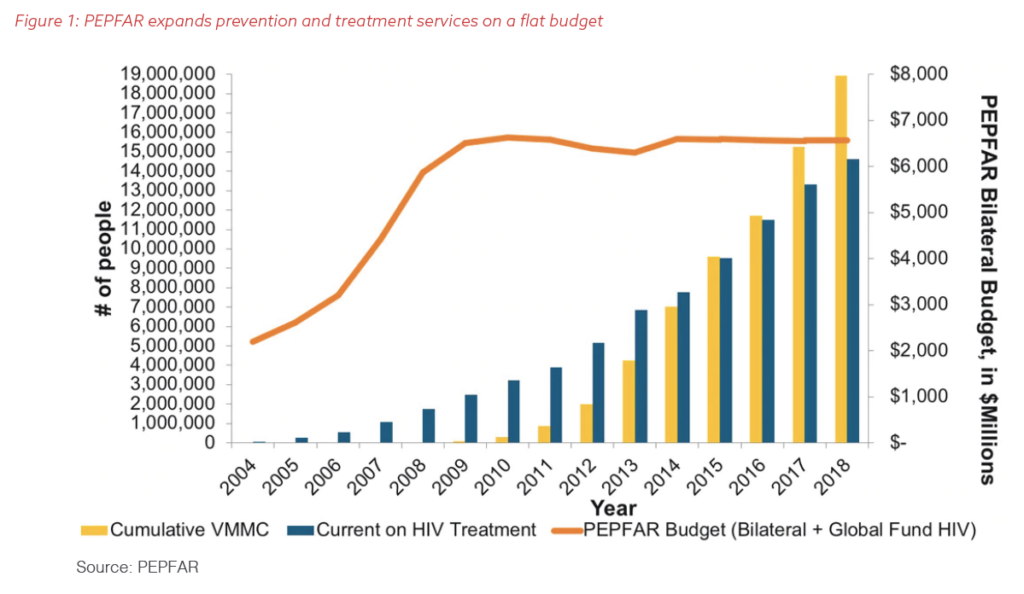
This report series examines the lessons PEPFAR offers. The first paper in this series discussed the critical importance of data and measurement to developing, managing, and improving programs. The second paper discussed the importance of collaboration, respect, and data sharing between funders, multilateral organizations, and implementers to ensure every dollar is used to achieve the best results, to eliminate duplication, and to align resources and policies in service to others. This paper will provide specific examples of how PEPFAR has deployed geolocation technology and sophisticated collection tools to generate data that drive better outcomes for its clients and methods that can revolutionize U.S. foreign assistance if applied more broadly. In an era of static budgets, PEPFAR has achieved incredible gains by analyzing localized information to track the HIV epidemic as it changes and efficiently deploying its resources to reach the right people in the right places (Figure 1).
PEPFAR has been continuously deploying site-level data to focus programming where the need is the greatest and to map the HIV epidemic and its trends. In addition to rebalancing its funding across the African continent based on the epidemiology of HIV, PEPFAR has taken deep geographic dives within each country to ensure its investments match both the risk and burden of disease and the need for, and access to, services.
Only this laser focus on matching geolocation, health, and demographic data allows PEPFAR to support the governments and people of the countries in which it works to meet two objectives: the “95/95/95” targets set by UNAIDS for 2030 (95% of people should know their HIV status, 95% of those HIV-positive should be taking lifesaving treatment, and 95% of those treated should have undetectable levels of virus in their blood) and the United Nations sustainable development goal to ensure healthy lives and promote well-being for all at all ages.
Download the report (PDF)
View recommendations
Evaluating progress in combating HIV/AIDS across countries
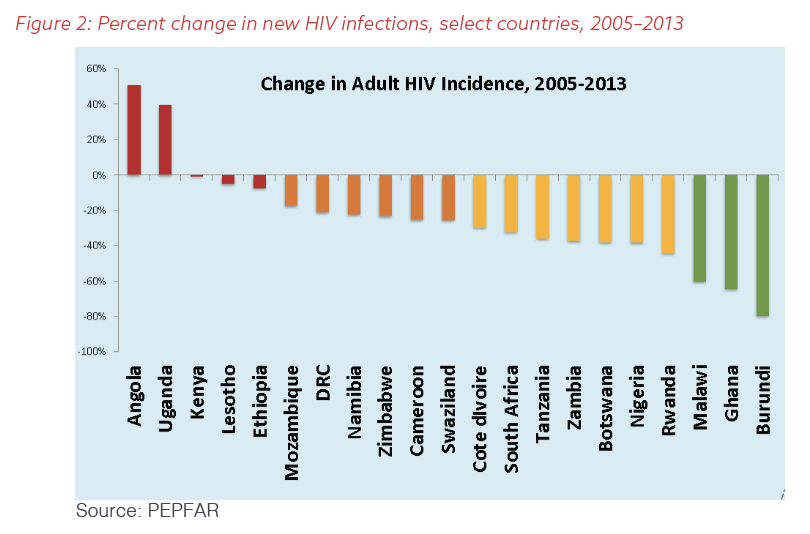
Programming across countries and continents enables the U.S. Global AIDS Coordinator to track PEPFAR’s outcomes and impact across the globe and to move past perceptions to work directly with communities in real time to prevent infections and save lives. This global perspective creates the ability to evaluate the program for comprehensive progress and to use data to understand its success and failures. Doing a deep data analysis in countries with greater progress helps identify lessons learned and translate them to ensure improvements in other places. With the reality of a flat budget and unequal progress across countries, as shown in Figure 2, the Office of the Global AIDS Coordinator, in collaboration with host governments, agencies, partners, and communities, reviews all aspects of the PEPFAR program on a continuous basis to align budgets with need and to ensure achievement of the global sustainable development goal to end AIDS.
Unlike most U.S. foreign-assistance programs, PEPFAR has gone beyond global analysis or even country-by-country comparisons, to identify progress in specific geographic communities to ensure funding and services focus on need and equity. This has only been possible because of the marriage of geolocation and site-level clinical data, district by district, county by county, everywhere PEPFAR works.
What is Geolocation?
Geolocation is the process of identifying where a person or object is via the satellite-enabled GPS. Geotagging attaches the location to a set of data.
PEPFAR’s Embrace of Geolocation Data for Decision-Making
The defining characteristic of PEPFAR since its launch has been its emphasis on the measurement of quantifiable results. In 2003, President George W. Bush and bipartisan majorities in Congress agreed on concrete initial goals for the program: reaching 2 million people with lifesaving treatment for AIDS; preventing 7 million new infections; and caring for 10 million children and adults either living with or affected by HIV, including orphans and vulnerable children (OVCs) who had already lost parents to the disease. The law that authorized PEPFAR, the Tom Lantos and Henry Hyde United States Global Leadership Against HIV/AIDS, Tuberculosis, and Malaria Act, called for reporting on progress every six months.
Early in the program’s rollout, PEPFAR faced limitations in fulfilling its mandate for measurement, as most sites initially were unable to meet the program’s expectation to break out data by sex or specific age bands. In most of the countries where PEPFAR works, patient records and information on stocks of medicines and medical supplies were kept on paper. Systems to report on cases of infectious diseases like HIV (called “surveillance”) were basic and limited in coverage – if they existed at all – and they did not exchange information with one another. With the exception of some federal countries in which states or provinces have direct responsibility for providing health care, governments only published national-level data on HIV. Therefore, the statistics on the numbers of people infected with HIV in the population as a whole (“prevalence”) and each year (“incidence”) were countrywide. Many governments did not know exactly how many public and private clinics and hospitals existed in their countries, or where they were.
Nevertheless, PEPFAR required partners to track the number of children and adult women on treatment – although initially only pregnant women who received a complete course of antiretroviral (ARV) medication in a program meant to prevent the transmission of HIV from mothers to their children (PMTCT). The program also counted women who completed counseling and testing.
As a result, PEPFAR achieved immediate success in reaching women, who were the majority of the beneficiaries of PEPFAR’s interventions in its early years. According to PEPFAR’s first annual report to Congress, issued in 2005, women made up almost 60% of the people who received treatment through PEPFAR and 69% of those who underwent testing and counseling for HIV. This pattern continued over the program’s first decade.
Yet even when broken down to the level of province or district, such aggregate numbers did not allow program managers and policymakers to allocate resources to the places that serve people at highest risk. Furthermore, these data also obscured poor performance, and excellence, among health care institutions and social-service providers. When PEPFAR made HIV treatment widely available, countrywide data did not permit the program to understand patterns of adherence with sufficient fidelity. It became obvious that some people were beginning their drug regimens, then stopping their pills after a few weeks or months, but PEPFAR and its partners did not have a good idea who these people were or why. Furthermore, PEPFAR only counted those reached for prevention and other services in broad terms and could not track individual OVCs under 14 or the impact of prevention messaging to individual outcomes from the general population.
In the early years of PEPFAR, it was a humanitarian imperative to scale up access to treatment to as many people as quickly as possible. Over time, data emerged that new infections were not equally distributed in each country, or even in localized subregions within them. These data led national and international implementers and thought leaders to publish a series of academic papers that reconsidered where and how new infections were occurring. They called for promoting changes in HIV programming to maximize access to lifesaving treatment and accelerate the potential for that treatment to reduce new infections.
The risk of acquiring HIV is not the same for everyone: Cultural and religious traditions and practices, access to health care and information, proximity to transportation networks, stigma and discrimination, individual behavior, and poverty, all of which can differ widely by location, can increase or decrease one’s risk. As a disease primarily contracted through sexual activity, HIV follows social networks not reflected in official government statistics. Because of the time lag between HIV infection and illness, outbreaks can spread quietly among marginalized and vulnerable people for months or years before detection. Therefore, national-level data can disguise large pockets of transmission – especially among people who live far from health-care facilities or in communities that face discrimination – and hide underserved areas. These national data also fail to “see” the communities that are making greater progress and might have lessons to teach. For example, countrywide statistics might suggest that 50% of all people living with HIV (PLHIV) are on treatment. In truth, this number is an average: One geographic area in a country could have 75% of PLHIV on antiretroviral therapy (ART), while another only 25%; or 75% of adult women could be on treatment, while only 25% of adult men are. In either case, the average would be 50% of total clients on treatment but would not account for geographic or demographic variances in the data.
The Office of the U.S. Global AIDS Coordinator, which manages PEPFAR, realized the disadvantages that this paucity of data imposed on the program. To succeed, PEPFAR needed to improve its understanding of what was happening at the local level: where its beneficiaries sought out treatment and prevention services, how transmission was changing in specific communities, and what organizations and institutions could help. PEPFAR had to know exactly where its partners were working and to connect those sites to data. The program needed more granular data so its partners could identify and learn from successes while pinpointing and fixing failures.
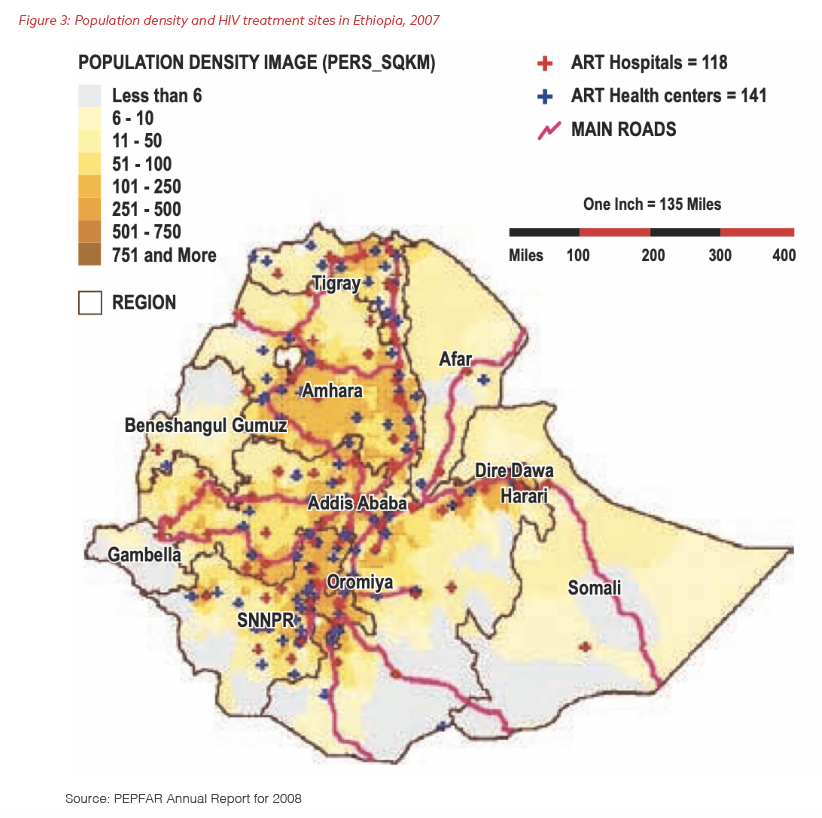
The solution was adding geolocation to epidemiologic and demographic data and investing in local systems to gather and analyze this information. In 2005, PEPFAR introduced geographic information systems (GIS) mapping and geospatial modeling to track changes in the epidemic and plan the introduction of services. In 2006, the Office of the Global AIDS Coordinator began requiring each PEPFAR country team to devote 7% of the budget of its Country Operational Plan to strategic information, including tools to track and use data generated at the site level. By 2007, PEPFAR was helping national governments to plot the location of sites that were providing treatment and care for HIV. Figure 3, a graph from PEPFAR’s Annual Report to Congress for 2008, is an early example of how the program began to combine information about treatment sites with census data on population density.
At the end of 2015, after several years of extensive consultation, data-collection (including information generated by PEPFAR support), and modeling, UNAIDS published “Focus on Location and Population,” a report that advocated for a shift in the approach to treatment to focus on the most-at-risk groups and geographic areas. Since PEPFAR from the beginning had required the reporting of granular data and invested heavily in collection and analysis so host governments and other partners could develop the systems to meet these reporting requirements, the program had a strong foundation to evolve once again. PEPFAR was ready to play a leadership role in responding to the growing shift in thinking and re-evaluate its allocation approach.
Throughout its first decade, PEPFAR moved funding between countries based on performance and epidemiology, but disparities in data meant that some countries with a high disease burden were receiving less than they should have been. Millions of people living with HIV or at risk of acquiring the disease were going without access to prevention tools, treatment, and care.
In addition to the mismatch at the regional level, the reliance on estimates and country-level data was beginning to produce distortions within each country. PEPFAR had been funding hundreds of sites based on modeling that was supposed to predict where HIV cases would emerge. But the program had trouble correlating case numbers to actual sites, and managers began to suspect that PEPFAR funding was not going to the places and people that needed it the most. Ten years into full implementation and in the fifth year of declining or flat annual budgets, PEPFAR needed to take further steps to ensure access and equity of needed services across all the countries where the program was investing its resources.
To fill these gaps in information, PEPFAR began gathering geolocation data for the specific sites where its partners were working beginning in 2014 and then made the collection mandatory two years later. Managers could now triangulate and match to actual physical locations the information gathered from censuses; multi-country analyses of HIV prevalence, incidence, and behavioral findings, called Population-Based HIV Assessment Surveys (PHIAs); and other surveys. The program also streamlined and boosted reporting to a quarterly schedule, increased to monthly reporting from sites that were significantly underperforming to ensure continuous data-driven improvements and actions that resulted in better outcomes. In addition, PEPFAR began tracking expenditures by site to understand which locations and organizations were using resources most efficiently. By 2017, PEPFAR was publishing all site-level data, disaggregated by age and sex, in a transparent format on PEPFAR.gov. More than a decade of investments in strategic information tools and systems with host-country governments and other partners made these reforms possible.
The result of this approach has been that PEPFAR, as part of its annual review process, began identifying sites that do not need resources because of changes in the local epidemic over the previous year. The program redirects resources away from them to hospitals, clinics, and other institutions that are diagnosing and treating more individuals living with HIV/AIDS and need expanded resources to address underserved and underfunded populations and areas. The methodology also identifies high-performing sites, which PEPFAR studies for valuable lessons that others can apply to improve.
Integrating these three data sources – survey and surveillance, program performance, and expenditure – offers an evidence-based alignment of resources and programs to most effectively strengthen the response to the epidemic.
– PEPFAR Annual Report to Congress for 2016
Illustrations of the importance of collecting and using GIS and local data to align PEPFAR’s programs and investments for maximum impact.
Kenya
Reporting location-linked data was revolutionary for PEPFAR’s model. By tracking progress by geographic coverage areas, PEPFAR can carry out even more effectively its longtime strategy of ensuring the services it funds are available and accessible to the right populations in the right places and reorient its funding accordingly.
A perfect example is what took place in Kenya. Beginning in 2014, the Office of the Global AIDS Coordinator did a deep dive into the clinical locations PEPFAR was funding in Kenya, starting with those focused on PMTCT. All sites were GIS mapped and required to begin collecting more specific numbers: pregnant women tested, those found to be HIV-positive, and those then supplied with critical interventions to treat HIV and prevent the infection of their babies both through pregnancy and breastfeeding.
Data analysis showed that sites and funding were not aligned in an equitable manner. To the great surprise of the Kenyan government and PEPFAR’s partners, 90% of HIV-positive patients came from fewer than one-third of the sites, and almost 2,000 hospitals and clinics had not identified even one HIV-positive mother in the previous year. Figure 4 illustrates these findings, first revealed in PEPFAR’s Semi-Annual Program Review for Kenya in 2014.
This extreme disparity left some sites overwhelmed with patients, while others were receiving funding and support for no clients. As the PEPFAR Annual Report to Congress for 2015 described the situation, many “HIV-positive women are not linked to necessary lifesaving services for themselves, and there is no way to ensure their babies are born HIV-free.”
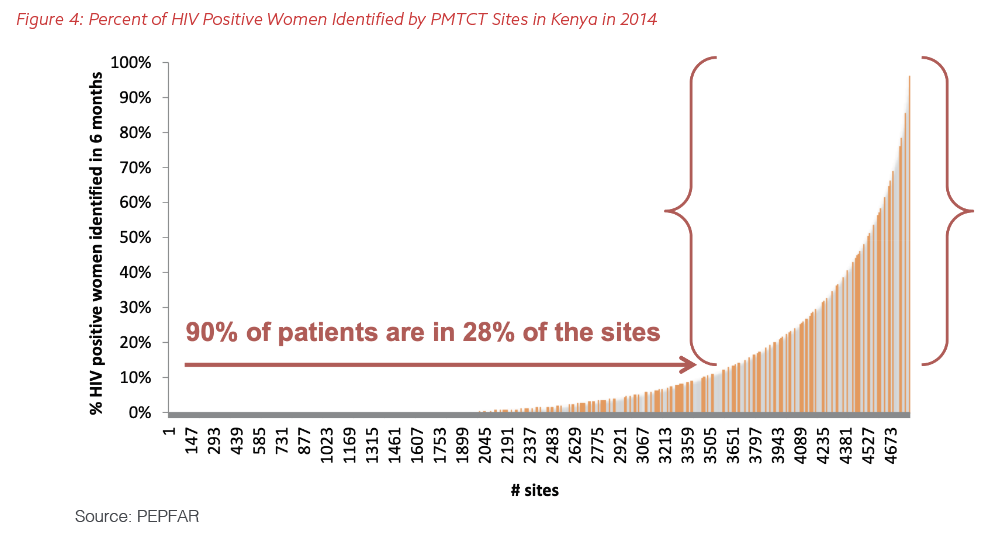
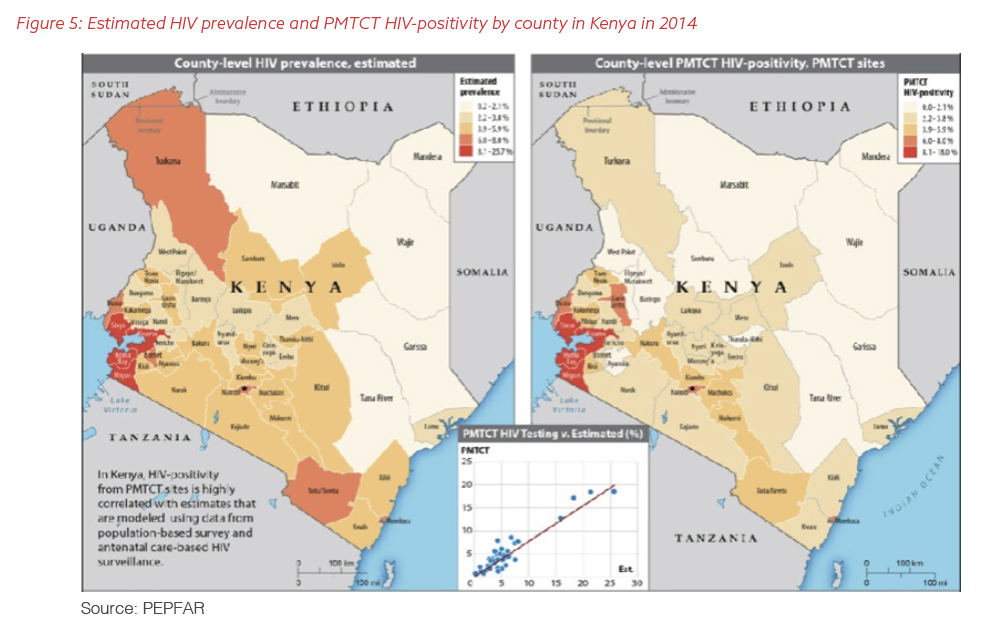
Figure 5 shows how PEPFAR triangulated county-level data in Kenya to show where the unaddressed needs were the greatest and program data that identified where HIV-positive patients were actually being detected and seeking treatment. The analysis showed the greatest need was in the Kisumu area around Lake Victoria.
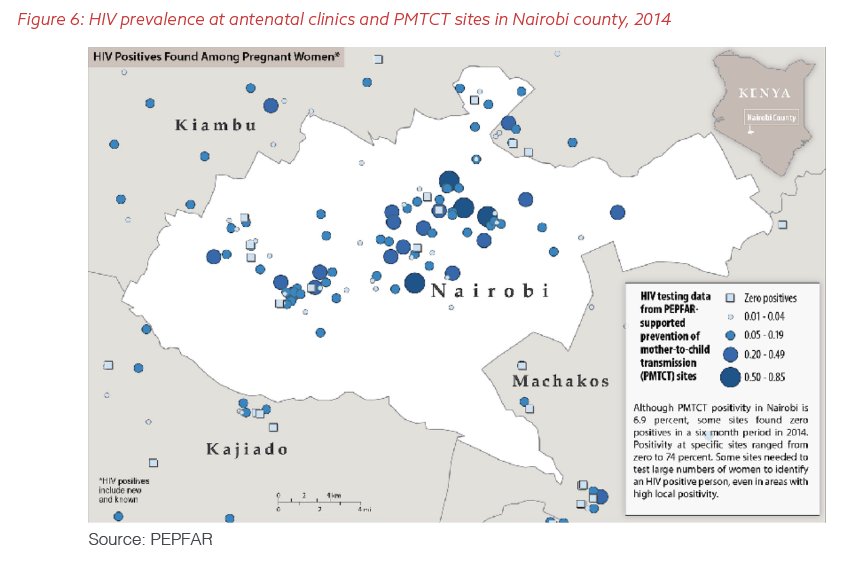
As Figures 6 shows, even highly populated areas in Kenya such as Nairobi had pockets of no or low transmission hidden in the previously available statistics. PEPFAR had invested resources in these locations for years, often at high cost, but with little impact. Consolidating and concentrating services at the sites that were testing and treating larger numbers of HIV-positive women offered an opportunity to increase PEPFAR’s impact by aligning the program’s resources to mirror the real, geographic-specific epidemic.
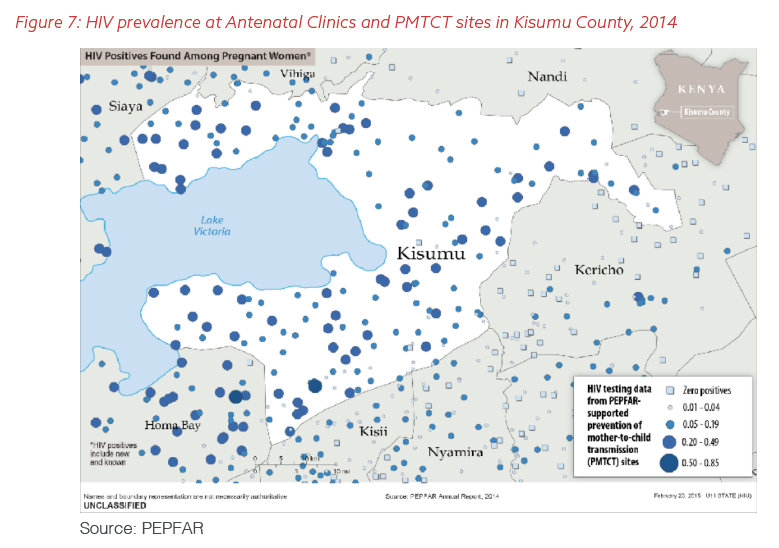
PEPFAR used the new data to reallocate its resources in Kenya to ensure those with the greatest need had access to both prevention and treatment services. In particular, the Office of the Global AIDS Coordinator aligned its investments based on demonstrated need and moved resources to the higher-prevalence areas of the Kisumu region on the shores of Lake Victoria (Figure 7).
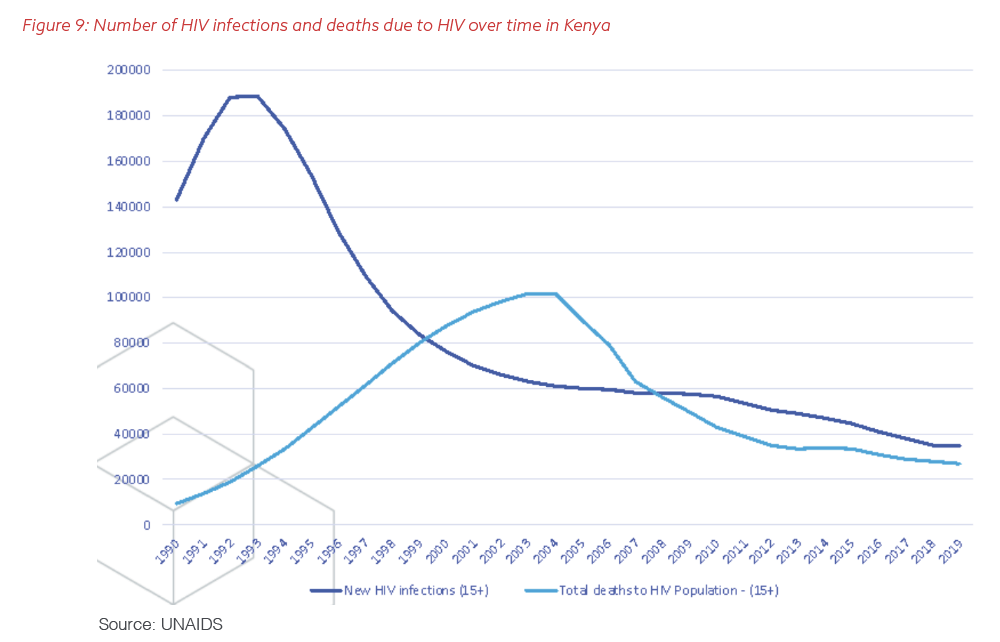
PEPFAR soon applied this geographic refocusing to hone its testing programs across all of the countries in which it was working to identify those at highest risk, empower them to know their HIV status, and link them to care when needed. As shown in Figure 8, PEPFAR shifted resources from 2014 to 2016 to the geographic areas that had been significantly underfunded previously and initiated new programming to address specific vulnerable groups, including expanded prevention interventions in the LGBTQ+ community and among young women. Overall, PEPFAR realigned nearly 25% of its funding in Kenya over those years, which resulted in an accelerated decline in new infections and further drove down fatalities, as demonstrated in Figure 9. Specific areas like Kisumu saw a dramatic improvement in access to prevention and treatment services and client-specific outcomes.

Tanzania
A similar process of requiring new data and deeper analysis helped PEPFAR ensure that its funding, focus, and comprehensive support programming all align for maximum impact on children’s lives. In 2014, the PEPFAR team in Tanzania began triangulating social services, clinical, and geographic data on PLHIV, children treated with ART, and OVCs who were receiving care. Figure 10 shows the mismatch the analysis revealed: PEPFAR’s partners were taking care of lots of OVCs in areas with low rates of pediatric HIV, which meant that the program was overlooking thousands of children who had lost a parent or caregiver to the disease in high-prevalence regions. The numbers for children on ART also brought into stark relief that PEPFAR had to be missing HIV-positive youngsters in the parts of Tanzania with the highest concentration of PLHIV, especially in the west and northwest of the country.
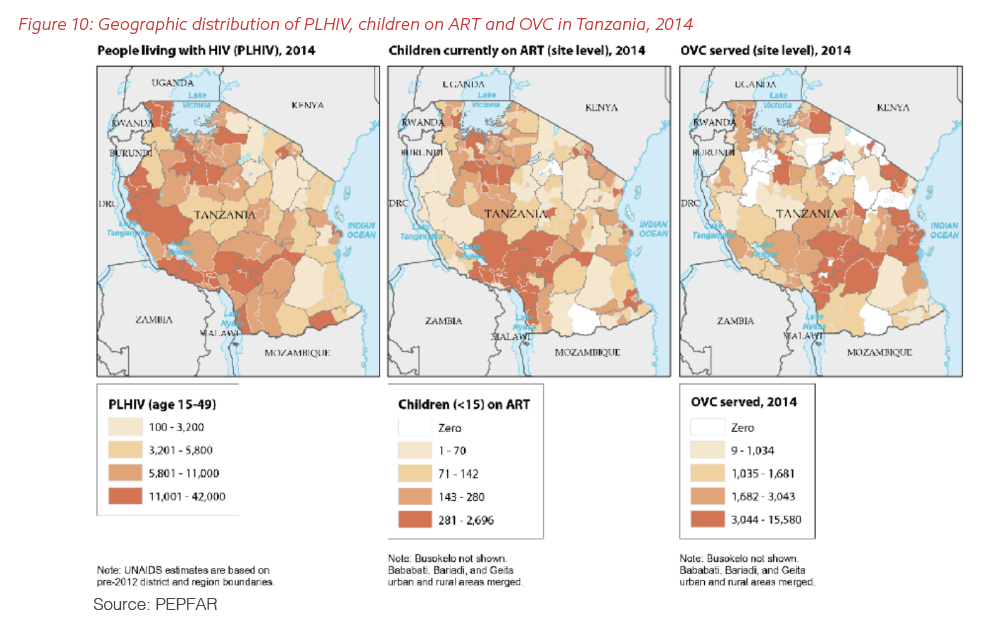
In Tanzania, PEPFAR relied on the new understanding brought about by harnessing geolocation, epidemiologic, and service-delivery data to redistribute resources. In a process similar to the one undertaken in Kenya for PMTCT, the PEPFAR team and its partners in Tanzania moved funds for OVCs to the regions with the highest prevalence of HIV while redoubling their efforts to find and bring into treatment HIV-positive children in those areas they had previously missed. At the same time, the Office of the Global AIDS Coordinator launched Accelerating Children Treatment (ACT) to ensure children could start lifesaving medicines and they and their families could receive psychosocial support services to ensure nutritional and structural support. Over just two years in Tanzania, PEPFAR doubled the number of children on ART, a pattern repeated across many countries.
Uganda
Uganda saw a sharp decline in deaths from AIDS during the first years of investments by PEPFAR and the Global Fund to Fight AIDS, Tuberculosis, and Malaria as access to treatment increased rapidly across the country. Plain-spoken leadership from the national government, community elders, religious figures, and PLHIV themselves helped drive the widespread uptake of ART, including through innovate home-delivery models.
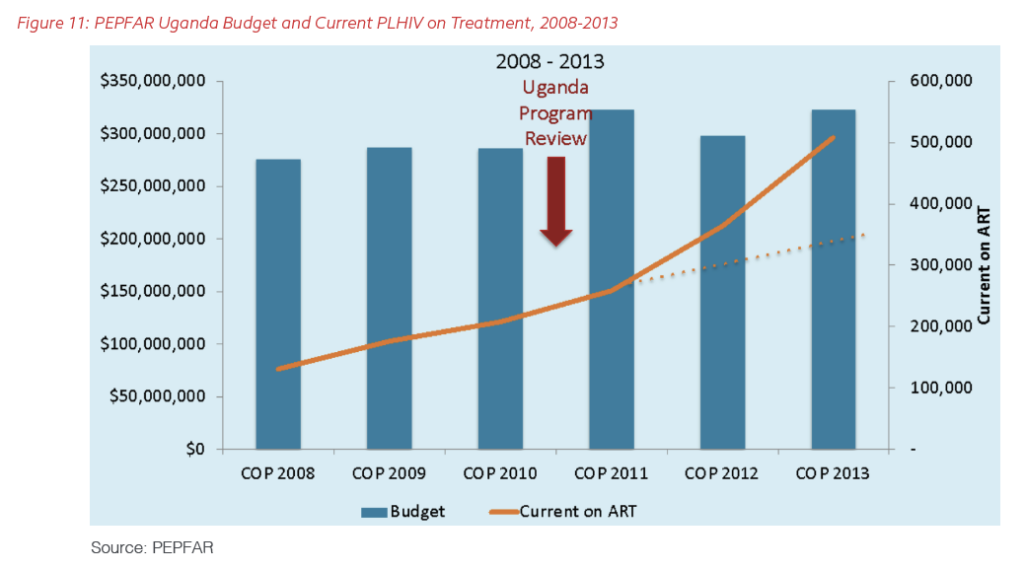
By 2009, however, the Ministry of Health, the Office of the Global AIDS Coordinator, and the PEPFAR team and partners in Uganda found their progress in controlling the pandemic had stalled: The pace of starting HIV-positive clients on ART was not keeping up with the epidemic in the country. Uganda therefore underwent the first programmatic realignment of resources for adult ART in 2010 and 2011. PEPFAR reexamined its spending to prioritize “core” interventions that would have the greatest direct impact on transmission, with treatment at the top of the list, and looked for areas where U.S. funds could have the greatest impact. According to the PEPFAR Annual Report to Congress from 2016, “The Uganda PEPFAR team ranked districts according to the number of [PLHIV] and found that 82% of [PLHIV] reside[d] in 61 of 111 total districts. This means that 45% of the districts serve[d] less than 18% of the burden.”
This exercise led to a reallocation of funding to focus on the areas with the greatest number of PLHIV and people at risk. As Figure 11 demonstrates, the PEPFAR team over the next two years used this approach to expand the number of people on ART in the country dramatically, despite a flat budget.
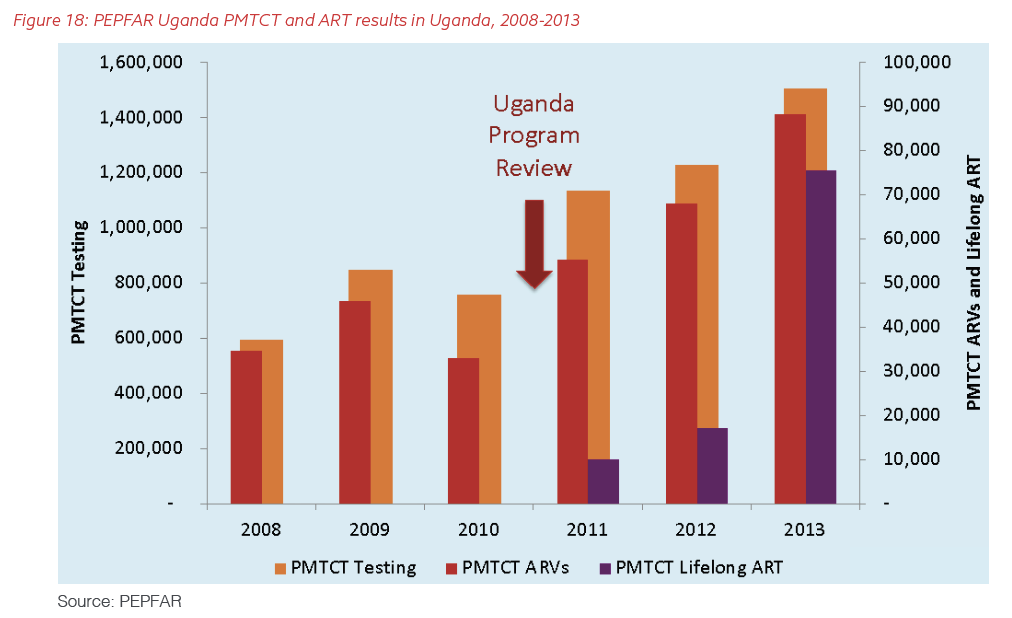
PEPFAR has continued to use detailed age bands to understand precisely who the program is missing, disaggregated by sex and connected to monthly reporting from GIS-tagged sites. Recent PEPFAR program data show that Uganda has demonstrated a marked improvement in both the numbers of people on ART and the success of their treatment (Figure 12 and 13). Year after year in Uganda, PEPFAR has created geospatial maps to show where the people who needed access to treatment live, how many are in treatment, and the gap. (See Figures 14, 15, and 16.) The program prioritizes funding to the regions with the highest need and the highest treatment deficits. PEPFAR performed similar analyses for key prevention services focused on a biomedical intervention for young men – voluntary medical male circumcision (VMMC) – and its DREAMS program for prevention in young women. A very data-driven Ugandan minister of health used this information in real time to advance critical new policies and ensure their implementation down to the site level.
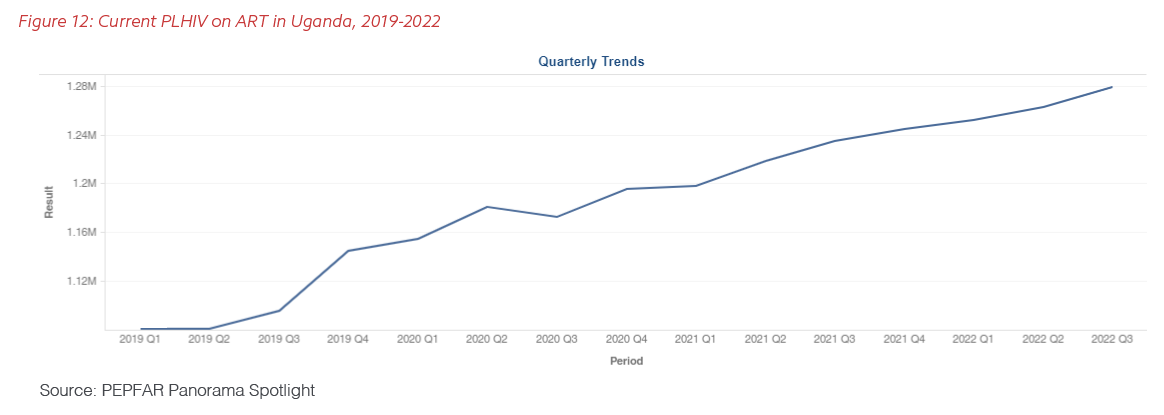
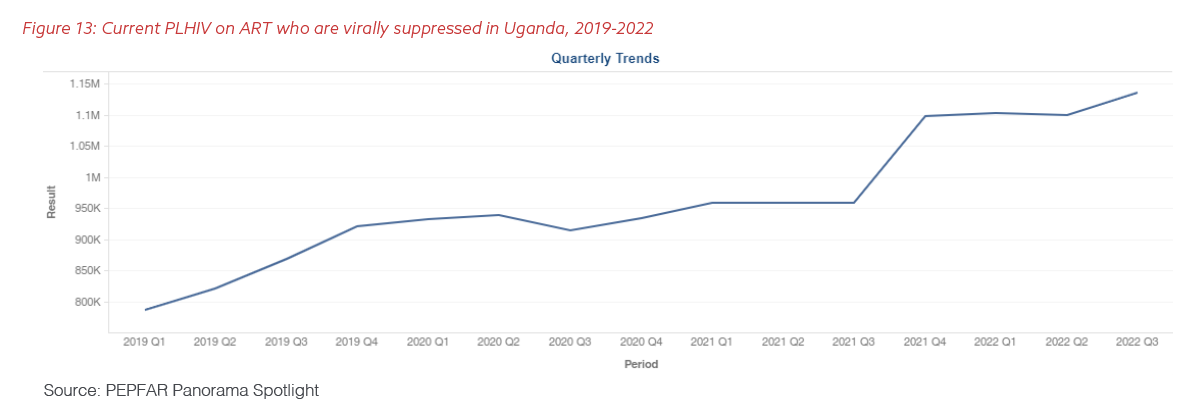
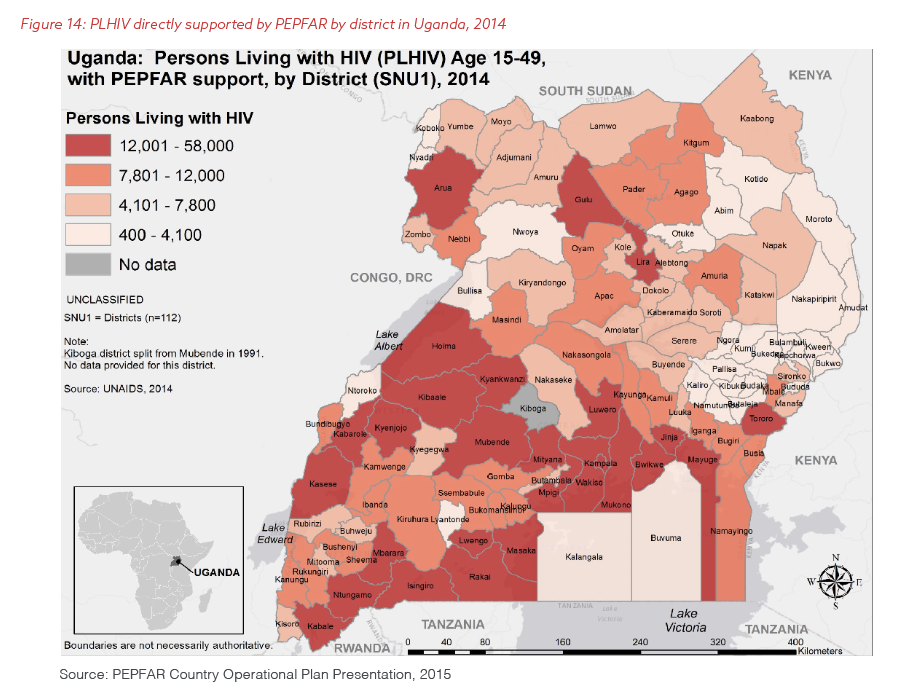
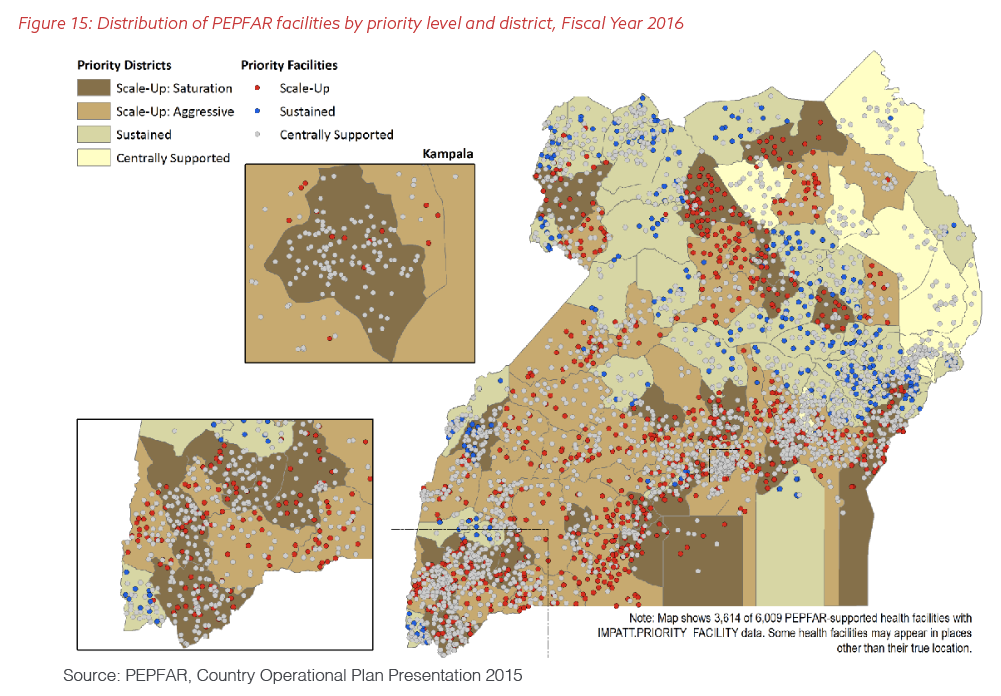
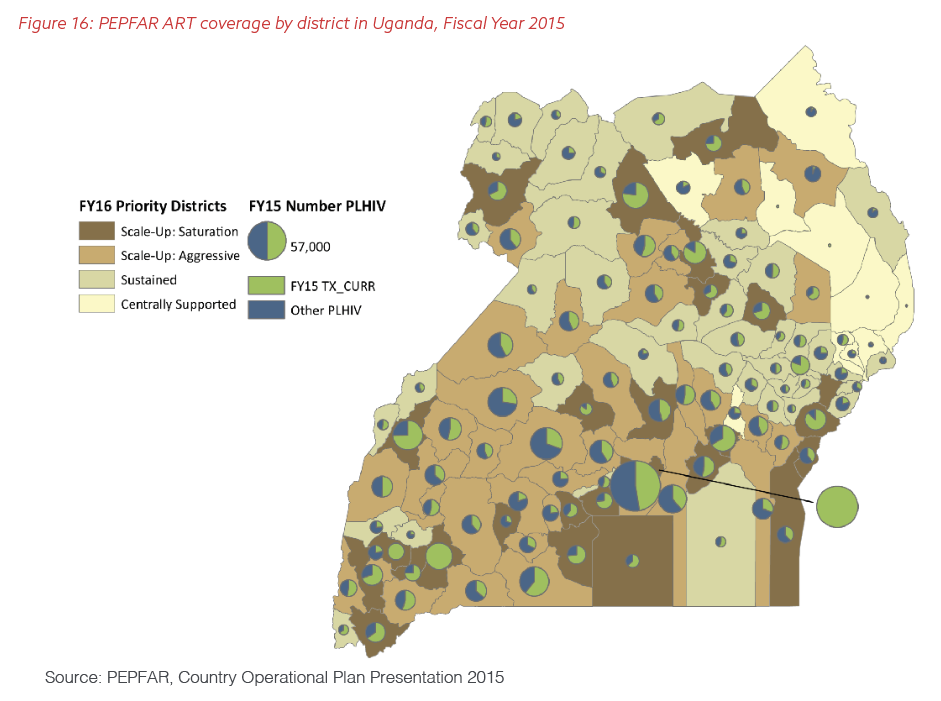
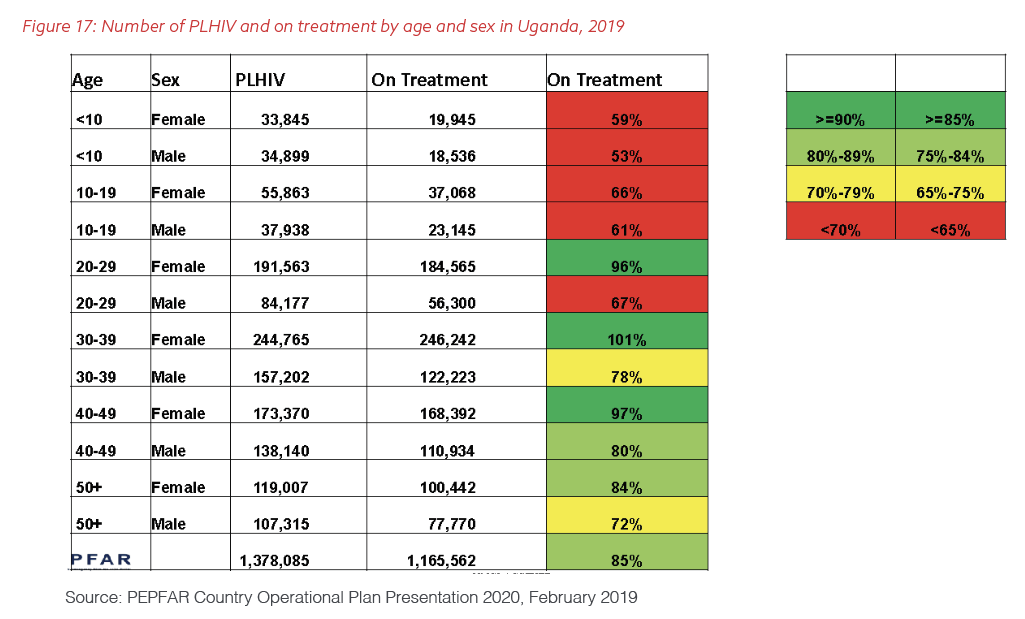
Figure 17 is an example of the internal PEPFAR charts that managers of the program have used to see the gaps between the number of people reported to have tested HIV-positive in Uganda and the number of clients known to be on ART, broken down by age and sex.
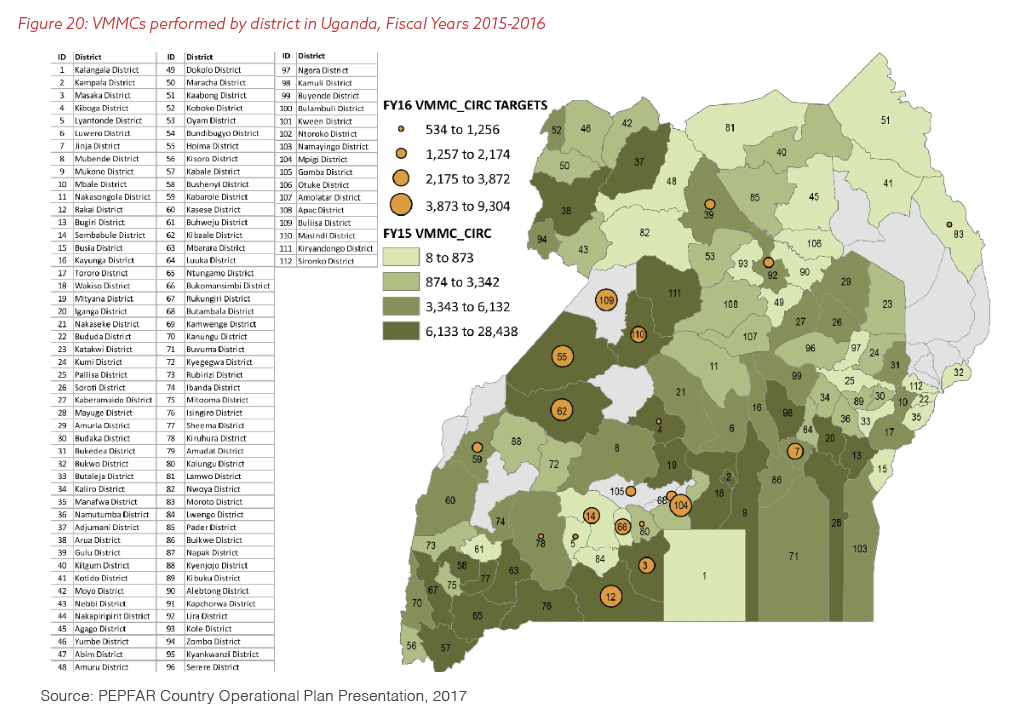
PEPFAR used the lessons from its programmatic review of ART performance to change its other core interventions in Uganda. As Figure 20 shows, examining new, site-level data allowed PEPFAR and its partners to shift resources to introduce the so-called “B-Plus” approach for HIV-positive pregnant women in Uganda, which places them on lifelong treatment as soon as they are diagnosed. As a result, seven times as many such women were on ART in Uganda by the end of 2013 than had been just two years before.
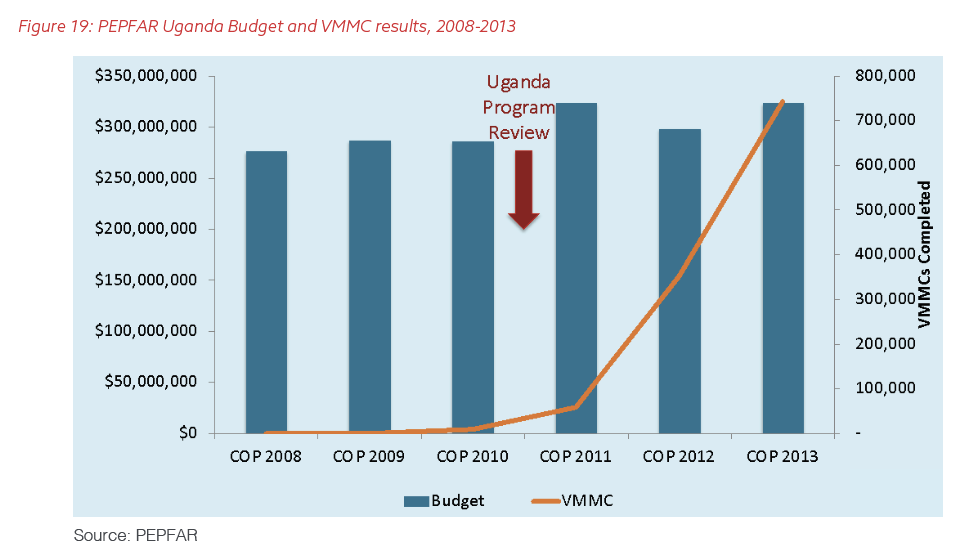
The savings from the more-efficient deployment of treatment also permitted PEPFAR to add VMMC to its core program in Uganda. Figures 19 and 20 show the explosive growth in this technique, which can reduce men’s risk of acquiring HIV through heterosexual sex by almost 60%, according to the World Health Organization.
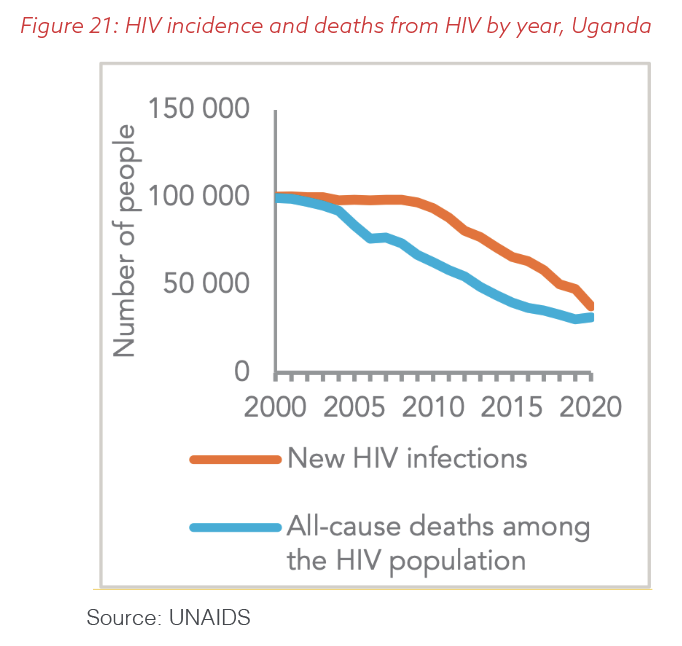
The Ugandan minister of health used the deep data dives to push policy reforms and harnessed site-level information to ensure the full implementation of the changes. In partnership with the Ministry of Health and local communities, programs funded by the Global Fund and PEPFAR used data for decision-making to extend the reduction in deaths from AIDS that had begun years before while improving the prevention of new infections, as shown in Figure 21. As a result, by 2019 Uganda achieved the “90/90/90” goals early across all age bands of adult women, approached them in adult men, and dramatically decreased the number of new infections and deaths, as detailed in the UNAIDS Data 2020 report.
Ensuring the accuracy and integrity of data
With so much riding on the numbers, how does PEPFAR make sure the data it uses are accurate? And how does PEPFAR prevent and root out fraud in reporting?
When pivoting to employing data so assertively to make decisions, the Office of the Global AIDS Coordinator realized that the incentives for abuse were too strong to rely only on partners’ self reporting. As a result, PEPFAR has adopted the approach of former President Ronald Reagan in pursuing arms-control agreements with the Soviet Union: “Trust, but verify.”
The Office of the Global AIDS Coordinator took a two-pronged approach. First, it funded PHIAs, for which an independent external group performed comprehensive, community-level HIV surveys to validate the prevalence and incidence of HIV and verify service-level data on testing, treatment, and prevention knowledge among clients. Second, the Office of the Global AIDS Coordinator revamped its internal policies and systems for quality control and quality assurance.
In 2014, PEPFAR initiated the most extensive push in the history of U.S. foreign assistance to improve the quality of site-level data, called the Site Improvement Through Monitoring System (SIMS). While visits to programmatic sites were nothing new for PEPFAR and many other programs, SIMS is a more streamlined and comprehensive process of assessing whether providers are following worldwide and national quality standards, both for the services they deliver and the data they collect. PEPFAR’s SIMS teams use standardized tools at health facilities and in the communities around them and also check the quality of the technical assistance partners are offering to sites.
Thousands of SIMS visits have taken place in the last eight years, the vast majority in health facilities, as well as in communities that connect beneficiaries to them. Despite a disciplined emphasis on quality assurance, the visits are not punitive inspections; they include supportive supervision for providers and checks on the status of infrastructure and stocks of medicines, health supplies, and equipment. The PEPFAR SIMS teams watch carefully for innovative clinical and managerial techniques that they can take to other sites to improve their performance and outcomes for clients.
The SIMS visits have been critical to preventing and spotting waste, fraud, and abuse. The close examination of results and the realities in the field have led the Office of the Global AIDS Coordinator to adjust payments to implementers and even switch partners if poor performance persists. In one notable case, based on anomalies first identified by SIMS teams, the organization responsible for the majority of VMMC sites in Zambia had to reimburse millions of dollars in PEPFAR funds to the U.S. Agency for International Development (USAID) because of inflated numbers of beneficiaries. PEPFAR at both the headquarters and country level cooperates closely with the Offices of the Inspector General at USAID, the U.S. departments of Health and Human Services and State, and the Global Fund.
The critical importance of diplomacy and clear communications
Aligning need with comprehensive programming requires the reallocation of budgets and investments. This means some geographies will receive more funds and others will receive less. Those that receive more never react publicly with positive messaging, as they are getting their fair share since they have a greater need, but those that lose money are very vocal. PEPFAR program managers and officials at U.S. embassies need to be prepared for this reality and work with governments and communities to ensure they understand the data and the “why” behind the budget adjustments. They should be encouraging partners which receive their appropriate allocation to present and publish about their experiences to show the positive outcomes of collecting and using data in the right ways.
At the same time, with greater funding comes greater expectations. The sites that receive more funding need higher targets and the expectation that they will serve more clients with prevention and treatment services and continue to collect data accurately to ensure progress is clear. PEPFAR posts all of its data on PEPFAR.gov, which allows access to everyone, including the beneficiaries, partners, governments, and communities. This transparency has driven better decision-making that has improved outcomes for clients and the U.S taxpayer.
Conclusion
Comprehensive, granular local data are critical for continuous improvement in global health and development programs. To be successful, managers of these initiatives at all levels, beginning with the host-country governments, must constantly increase the depth, breadth, and uniformity of the data collected; refine definitions to ensure consistency of collection; and eliminate data collection that is no longer valuable. They must also use the refined data to adjust their budgets and realign their investments, a process that results in more clients reached with quality services and improved outcomes and impact.
Programs cannot be established and then go on autopilot or rely on modeled data reported every two or four years. Granular data allow all program managers at all levels, beginning in implementing countries, to see and understand success and translate key innovations across sites to improve service delivery. Granular data also permit managers to see sites that are struggling and need additional support and, potentially, increased funding.
When battling pandemics locally, one must constantly use data to improve programmatic implementation in real time. Annual analyses of data are too slow: They lead to unnecessary new infections and death. Real-time data, especially disaggregated granular data matched to geolocation information, are needed to ensure programs are continuously evaluating the quality of their services, the access to those services by the right populations, and how to remove barriers to care.
PEPFAR did not invent geolocation, nor was it the first health program to implement it. But no U.S. foreign-assistance initiative has been as successful in using an open, transparent, data-driven approach that strategically targets geographic areas and populations to achieve the greatest impact. Based on 20 years of experience, PEPFAR’s collection and visualization of data continue to evolve based on the unique programmatic needs in each country, and, within each country, each region and population. The Office of the Global AIDS Coordinator continues to prioritize data for decision-making and upgrade systems for this purpose. The program has driven the collection of data down to the site level, at individual hospitals, clinics, and other facilities identified by GIS coordinates, and combined streams of health and demographic data with mapping. Supported by intensive quality assurance and supportive visits to each service-delivery location, this methodology has permitted PEPFAR to adjust its funding and geographic focus to find people the program had previously missed and achieve efficiencies to expand treatment, care, and prevention services even without budget increases. All U.S. foreign-assistance programs related to global health and development should adopt this approach.
“Earth observation is no longer just a way to satisfy our curiosity but has become crucial in ensuring the survival of humankind.”
– Former South African Minister of Science and Technology Mosibudi Mangena, 2007
Recommendations
The United States should learn from PEPFAR’s real-time use of geolocation data and data analytics to improve the U.S. government’s assistance:
Congress
- Congress should amend the Foreign Assistance Act and the Government Performance Reporting Modernization Act to require all recipients of U.S. foreign-assistance programs related to global health and development that are supporting individual service-delivery sites to collect geospatial coordinates for each location.
U.S. government departments and agencies that implement foreign assistance related to global health
- These departments and agencies should update their regulations and internal policies to require that programs in health and nutrition, agriculture, environmental protection, climate adaptation, education, and other site-specific fields match each site of activity with geospatial coordinates and have clear, site-level metrics to track outcomes and impact.
- Implementers should also collect and report data that have stripped of specific individual identifiers, at each site regularly and consistently. Working with host governments and communities, local teams should use these real-time data to track progress against clear metrics to ensure sustainable outcomes and impact.
- They should prioritize field visits in their plans for monitoring and evaluating all site-based activities and create standardized systems like SIMS for conducting such visits and using data to improve programs continuously, increase their impact, and learn from sites with better outcomes.
- They should support regular, independent, community-level surveys to ensure the validity of program data.
Acknowledgements
The Bush Institute would like to thank Dr. Mark Dybul, former Executive Director of The Global Fund (2013-2017) and former U.S. Global AIDS Coordinator (2006-2009), and Dr. Jen Kates, Senior Vice President and Director of Global Health & HIV Policy at Kaiser Family Foundation, for their insightful feedback on and review of this paper.





























